ROBOTIC LAPAROSCOPIC SADI S - SLDS
-
Dr. AMAR VENNAPUSA
ROBOTIC, LAPAROSCOPIC
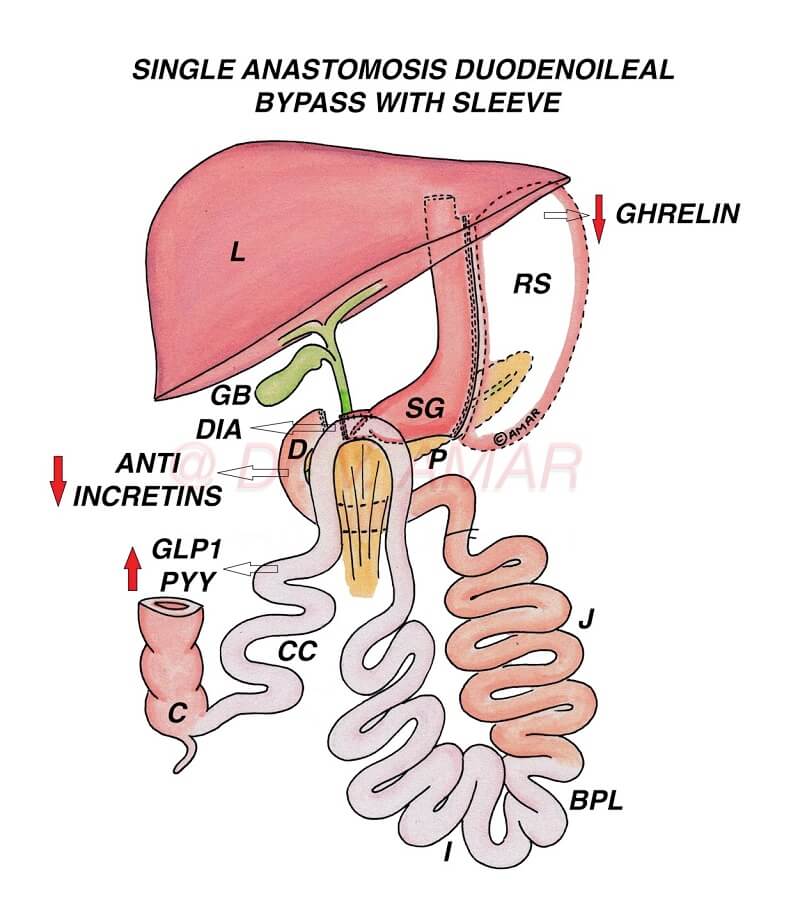
SINGLE ANASTOMOSIS DUODENOILEAL BYPASS WITH SLEEVE (SADI S)
SLEEVE WITH LOOP DUODENAL SWITCH (SLDS)
ONE ANASTOMOSIS DUODENAL SWITCH (OADS)
SINGLE ANASTOMOSIS DUODENAL SWITCH (SADS)
STOMACH INTESTINE PYLORUS SPARING SURGERY (SIPS)
-
Dr. AMAR VENNAPUSA
– It is one of the most advanced and effective bariatric & metabolic surgery for the treatment of severe obesity and severe diabetes.
– This and Duodenal Switch are the most powerful sleeve plus bypass combination surgeries (Sleeve plus procedures).
– Physiological changes are significantly high in SADI S, compared to standard bariatric & metabolic surgeries.
– It is a loop modification of biliopancreatic diversion with duodenal switch (BPD DS).
1. Performed by robotic or laparoscopic method (By putting small holes over the tummy) using advanced high quality imported laparoscopic equipment and instruments.
2. Up to 80% of the stomach is removed using high quality staplers and stapler guns to form a vertical sleeve.
3. When the stomach is divided using staplers, it is stapled in three rows, sealed and cut simultaneously.
4. The percentage of the removed stomach is relative but the capacity of the remaining gastric sleeve is 60 to 100 ml.
5. 1st part of the Duodenum (First part of the small intestine) is divided and anastomosed (joined) to the distal ileum (Last part of small intestine) in a loop fashion (Loop duodenoileal anastomosis). Approximately 50% of the small intestine is bypassed. Anastomosis can be performed by hand sewn (sutured) method or stapled method.
6. Small intestine before anastomosis (From ‘Duodenojejunal Flexure [Junction of Duodenum and Jejunum] to the Anastomosis) is known as ‘Biliopancreatic Limb’ and after anastomosis (From the anastomosis to the Ileocecal Junction [Junction of Small and Large Intestine]) is known as ‘Common Channel’
7. Common Channel length is generally kept at 250 to 300 cm. But I perform fixed percentage bypass (50% in majority) and keep longer common channel in order to minimise malabsorption without compromising on the efficacy. Anastomosis is midway between duodenojejunal flexure and ileocecal junction – 50:50 bypass.
As per IFSO Guidelines 2022
– In India and Asia,
1. Individuals suffering from mild obesity with the body mass index is ≥ 27.5 kg/m2 with co-morbid medical conditions such as uncontrolled type 2 diabetes.
2. Individuals suffering from severe obesity with the body mass index is ≥ 32.5 kg/m2 even without any co-morbid medical conditions.
– In Western countries
1. Individuals suffering from mild obesity with the body mass index is ≥ 30 kg/m2 with co-morbid medical conditions such as type 2 diabetes.
2. Individuals suffering from severe obesity with the body mass index is ≥ 35 kg/m2 even without any co-morbid medical conditions.
– Weight loss is mainly due to physiological changes altering body energy balance.
– Because of these changes
1. Appetite (Hunger) is reduced.
2. Metabolic rate is increased.
3. Energy expenditure is increased.
4. ‘Fat mass’ is reset to a lower level.
5. Fat starts melting as body doesn’t want to store large quantity of fat.
6. You don’t eat large quantity of food as you start hating unhealthy foods.
– Physiological changes are significantly high as undigested food directly enters the distal ileum.
– Diversion of the biliopancreatic juices contribute further to these physiological changes.
– Role of food restriction and malabsorption is secondary.
– Same physiological changes are responsible for type 2 diabetes remission.
1. Insulin resistance is reduced.
2. Insulin production is optimised to control blood sugars.
– Average excess weight loss is > 90%.
– Some may lose above average, even 100% of the excess weight loss.
– For Example – If you are 50 kg excess weight, you lose approximately > 45 kg on average. Some may lose all the extra 50 kg.
– Generally if your weight burden is less, you lose more percentage of excess weight and if your weight burden is more you lose less percentage of excess weight.
– Average Total weight loss percentage > 40%.
– Average diabetes remission is > 90%.
– It is necessary to follow lifestyle modifications to improve weight loss and diabetes remission and to prevent weight regain and diabetes recurrence.
– Results in long lasting and significant weight loss.
– Results in long lasting and effective diabetes remission.
– Physiological changes are very high in Sleeve with loop duodenal switch as longer small intestine is bypassed compared to the standard Gastric sleeve (SG), Roux en y gastric bypass (RYGB) or mini gastric bypass – one anastomosis gastric bypass (MGB – OAGB), and Sleeve with bypass combination procedures such as Sleeve with loop duodenojejunal bypass (SG LDJB) or Sleeve with proximal jejunal bypass (SG PJB), Sleeve with jejunoileal anastomosis (SG JIA) or Single Anastomosis Sleeve Ileal Bypass (SASI Bypass).
– Weight loss is more effective & long lasting after SADI S compared to the standard SG, RYGB or MGB, and Sleeve with bypass combination procedures such as SG LDJB, SG PJB, SG JIB, SASJ Bypass or SASI Bypass.
– Diabetes remission is significantly high & durable after Single anastomosis duodenoileal bypass with sleeve compared to the standard SG, RYGB or MGB – OAGB, and Sleeve with bypass combination procedures such as SG LDJB, SG PJB, SG JIB, SASJ Bypass or SASI Bypass.
– Average weight regain after Sleeve with loop duodenal switch is very low (< 5%).
– Average diabetes recurrence after SADI S is very low (< 5%).
– SADI S has several advantages compared to RYGB and MGB – OAGB.
1. There is no ‘at risk’ stomach remnant.
2. Calcium and iron deficiency risk is low since first part of the duodenum is not bypassed
3. Risk of dumping syndrome is less because of intact pylorus controlling food out put
4. There is no risk of marginal ulcers
5. Risk of internal hernias is low.
– Compared to BPD DS, protein energy malnutrition and malabsorption risk is low because common channel (intestine available for digestion and absorption) is relatively long.
– SADI S is technically more advanced, compleex and time taking compared to SG,
RYGB and MGB – OAGB. – It needs advanced laparoscopic surgical skills and training.
– There is loss of endoscopic access to biliary tract (Pathway connecting liver and small intestine).
– Protein energy malnutrition, malabsorption, foul smelling oily stools, diarrhea and incontinence are high if the common channel length is 250 cm or less. These problems are significantly reduced but efficacy remains same when common channel is kept minimum of 300 cm and bypassed small intestine of not more than 55%.
– Some may lose below average. Inadequate weight loss < 1%. They may lose only 5 to 10 kg and stop losing further.
– If anyone regains weight or if diabetes recurs after Sleeve Gastrectomy or Gastric Bypass, revision to Loop duodenal switch with 250 cm or Duodenal switch re-induce significant weight loss and diabetes remission.
– It is very very safe procedure.
– It is a life saving surgery.
– Severe obesity and severe diabetes are dangerous.
– Bariatric and Metabolic surgeries are very safe.
– Complications are very rare. Even if they occur, they can be rectified.
Publication in the World Journal of Laparoscopic Surgery (WJOLS) –
Vennapusa Amar, Panchangam Ramakant Bhargav, Kesara Charita, Chivukula Tejaswi. Safety and Feasibility of Laparoscopic Sleeve Gastrectomy with Loop Duodenal Switch Surgery for Obesity in Indian Patients.
World J Lap Surg 2020; 13 (3):117-124.
https://www.wjols.com/doi/WJOLS/pdf/10.5005/jp-journals-10033-1423
Please download the full text of the article from the above link
Publication in Revista Chirurgia Romania Journal.
Amar Vennapusa, Ramakanth Bhargav Panchangam, Charita Kesara, Gitika Raj Vyshnavi Vanta, Aishwarya Reddy Sannareddy. Analysis of weight-loss outcomes following laparoscopic one anastomosis duodenal switch. Chirurgia (2021) 116: 300-311, No. 3, May-June.
Please download the full text of the article from the above link
Publication in Diabetes & Metabolic Syndrome: Clinical Research & Reviews (DMS CRR) –
Amar Vennapusa, Ramakanth Bhargav Panchangam, Charita Kesara, Gitika Raj Vyshnavi Vanta, Mukharjee Syam Sundar Madivada. Metabolic efficacy following laparoscopic sleeve gastrectomy with loop duodenal switch surgery for type 2 diabetes in Indian patients with severe obesity. Diabetes & Metabolic Syndrome: Clinical Research & Reviews Volume 15, Issue 2, March–April 2021, Pages 581-587.
https://doi.org/10.1016/j.dsx.2021.02.036
https://authors.elsevier.com/a/1ciVj6fWV2ftRR
Please download the full text of the article from the above links