SLEEVE GASTRECTOMY WITH LOOP DUODENOJEJUNAL BYPASS
(SG LDJB)
-
Dr. AMAR VENNAPUSA
ROBOTIC, LAPAROSCOPIC
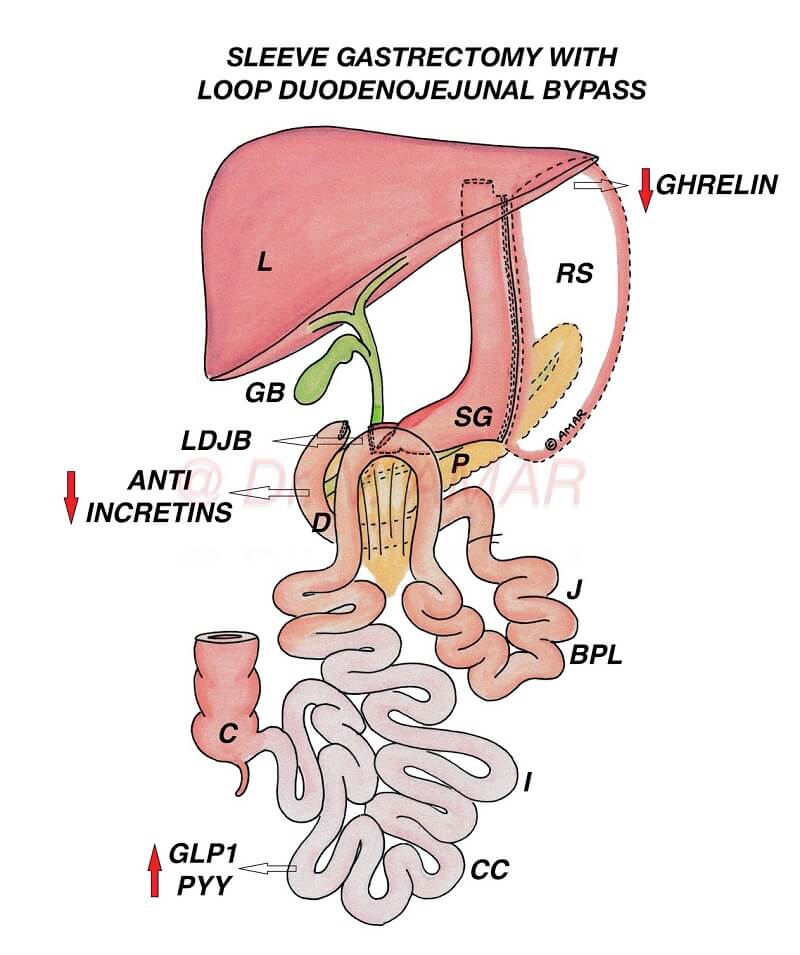
SLEEVE GASTRECTOMY WITH LOOP DUODENOJEJUNAL BYPASS
(SG LDJB)
-
Dr. AMAR VENNAPUSA
– It is a type of sleeve plus bypass combination surgery (Sleeve plus procedure) for the treatment of severe obesity and severe diabetes.
– It is a loop modification of biliopancreatic diversion with duodenal switch (BPD DS).
– It is similar to Single anastomosis duodenoileal bypass with sleeve (SADI S) but with a more proximal anastomosis (duodenojejunal anastomosis in place of duodenoileal anastomosis).
– Procedure:
- Performed by robotic or laparoscopic method (By putting small holes over the tummy) using advanced high quality imported laparoscopic equipment and instruments.
- Up to 80% of the stomach is removed using high quality staplers and stapler guns to form a vertical sleeve.
- When the stomach is divided using staplers, it is stapled in three rows, sealed and cut simultaneously.
- The percentage of the removed stomach is relative but the capacity of the remaining gastric sleeve is 60 to 100 ml.
- Duodenum (First part of the small intestine) is divided and attached to the mid jejunum (Second part of the small intestine) in a loop fashion 200 to 250 cm distal to duodenojejunal junction (loop duodenojejunal bypass).
As per IFSO Guidelines 2022
– In India and Asia,
1. Individuals suffering from mild obesity with the body mass index is ≥ 27.5 kg/m2 with co-morbid medical conditions such as uncontrolled type 2 diabetes.
2. Individuals suffering from severe obesity with the body mass index is ≥ 32.5 kg/m2 even without any co-morbid medical conditions.
– In Western countries
1. Individuals suffering from mild obesity with the body mass index is ≥ 30 kg/m2 with co-morbid medical conditions such as type 2 diabetes.
2. Individuals suffering from severe obesity with the body mass index is ≥ 35 kg/m2 even without any co-morbid medical conditions.
– Weight loss is mainly due to physiological changes altering body energy balance.
– Because of these changes
- Appetite (Hunger) is reduced.
- Metabolic rate is increased.
- Energy expenditure is increased.
- ‘Fat mass’ is reset to a lower level.
- Fat starts melting as body doesn’t want to store large quantity of fat.
- You don’t eat large quantity of food as you start hating unhealthy foods.
– Physiological changes are significantly high as undigested food directly enters from 1st part of the duodenum into mid jejunum and rapidly reaches distal ileum.
– Diversion of the biliopancreatic juices contribute further to these physiological changes.
– Role of food restriction and malabsorption is secondary.
– Same physiological changes are responsible for type 2 diabetes remission.
- Insulin resistance is reduced.
- Insulin production is optimised to control blood sugars.
– Average excess weight loss is ~ 70 to 80%.
– Some may lose above average, even 100% of the excess weight loss but that number is less.
– For Example – If you are 50 kg excess weight, you lose approximately 35 to 40 kg on average. Some may lose all the extra 50 kg but that number is less.
– Generally if your weight burden is less, you lose more percentage of excess weight and if your weight burden is more you lose less percentage of excess weight.
– Total weight loss percentage is ~ 30 to 35%.
– Average diabetes remission ~ 70 to 80%.
– It is necessary to follow lifestyle modifications to improve weight loss and diabetes remission and to prevent weight regain and diabetes recurrence.
– Results in long lasting weight loss.
– Results in long lasting diabetes remission.
– Physiological changes are relatively high in Sleeve with loop duodenojejunal bypass as longer small intestine is bypassed compared to the standard Gastric sleeve (SG), or Roux en y gastric bypass (RYGB).
– Weight loss is more effective & long lasting after SG LDJB compared to the standard SG, or RYGB.
– Diabetes remission is relatively high & durable after Sleeve with Loop duodenojejunal bypass compared to the standard SG, or RYGB.
– Weight regain after SG LDJB is low.
– Diabetes recurrence after SG LDJB is low.
– SG LDJB has several advantages compared to RYGB and MGB – OAGB.
- There is no ‘at risk’ stomach remnant.
- Calcium and iron deficiency risk is low since first part of the duodenum is not bypassed
- Risk of dumping syndrome is less because of intact pylorus controlling food out put
- There is no risk of marginal ulcers
- Risk of internal hernias is low.
– Compared to BPD DS, protein energy malnutrition and malabsorption risk is low because common channel (intestine available for digestion and absorption) is relatively long.
– SG LDJB is technically more advanced, complex and time taking compared to SG, RYGB and MGB – OAGB.
– It needs advanced laparoscopic surgical skills and training.
– There is loss of endoscopic access to biliary tract (Pathway connecting liver and small intestine).
– SG LDJB is less effective compared to Sleeve gastrectomy with loop gastroileal bypass (SG LGIB), SADI S and BPD DS because bypassed small intestine (biliopancreatic limb) is relatively shorter.
– Some may lose below average. Inadequate weight loss ~ 10%. They may lose only 5 to 10 kg and stop losing further.
– Average weight regain ~ 20 to 30%.
– Diabetes recurrence after SG LDJB is ~ 30 to 40%.
– If anyone regains weight or if diabetes recurs after Sleeve with Loop duodenojejunal bypass, revision to Loop duodenal switch or Duodenal switch re-induce significant weight loss and diabetes remission.
– It is very very safe procedure.
– It is a life saving surgery.
– Severe obesity and severe diabetes are dangerous.
– Bariatric and Metabolic surgeries are very safe.
– Complications are very rare. Even if they occur, they can be rectified.
Publication in the Journal of Minimally Invasive Surgery (JMIS) –
Amar Vennapusa, Ramakanth Bhargav Panchangam, Charita Kesara, Nazneen Mallick. Safety and feasibility of laparoscopic sleeve gastrectomy with loop duodenojejunal bypass for obesity. Journal of Minimally Invasive Surgery 2021; 24(1): 10-17. https://doi.org/10.7602/jmis.2021.24.1.10
http://www.e-jmis.org/journal/download_pdf.php?doi=10.7602/jmis.2021.24.1.10
Please download the full text of the article from the above link
Publication in Journal of Obesity and Metabolic Syndrome (JOMES) –
Amar Vennapusa, Ramakanth Bhargav Panchangam, Charita Kesara, Tejaswi Chivukula. Factors Predicting Weight Loss after “Sleeve Gastrectomy with Loop Duodenojejunal Bypass” Surgery for Obesity. JOMES 2020;29:208-214. https://doi.org/10.7570/jomes20044
http://www.jomes.org/journal/download_pdf.php?doi=10.7570/jomes20044
Please download the full text article from the above link
Publication in the Journal of Metabolic and Bariatric Surgery (JMBS) –
Amar Vennapusa, Ramakanth Bhargav Panchangam, Charita Kesara, Mukharjee Syam Sundar Madivada. Metabolic Efficacy and Diabetes Remission Predictors Following Sleeve Gastrectomy with Loop Duodenojejunal Bypass Surgery. J Metab Bariatr Surg 2020;9:33-41. https://doi.org/10.17476/jmbs.2020.9.2.33
http://www.jmbs.or.kr/journal/download_pdf.php?doi=10.17476/jmbs.2020.9.2.33
Please download the full text of the article from the above link
Publication in Journal of Obesity and Metabolic Syndrome (JOMES) –
Amar Vennapusa, Ramakanth Bhargav Panchangam, Charita Kesara, Tejaswi Chivukula. Response: Factors Predicting Weight Loss after “Sleeve Gastrectomy with Loop Duodenojejunal Bypass” Surgery for Obesity (J Obes Metab Syndr 2020;29:208-14). JOMES 2020;29:327-329. https://doi.org/10.7570/jomes20132
https://www.jomes.org/journal/download_pdf.php?doi=10.7570/jomes20132
Please download the full text of the article from the above link